PAH
WHO GROUP 1* 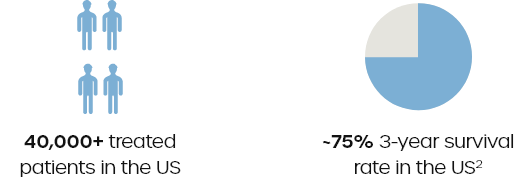
*WHO Group 1 refers to PAH, which is caused when the arteries in the lungs become narrowed, thickened, or stiff. As a result, the right side of the heart must work harder to push blood through these arteries.2
PH-ILD
WHO GROUP 3* 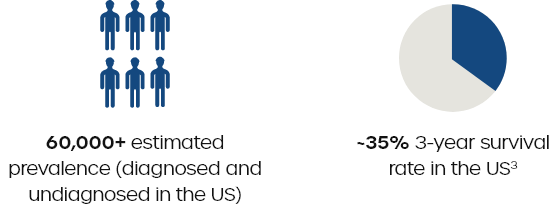
*WHO Group 3 includes PH due to chronic lung disease. PH-ILD includes a diverse collection of up to 150 different pulmonary diseases, including interstitial pulmonary fibrosis (IPF), chronic hypersensitivity pneumonitis, connective tissue disease (CTD)–related ILD, and chronic pulmonary fibrosis with emphysema (CPFE), among others.3
Focusing on the potential of inhaled treprostinil
Treprostinil is one of the most widely used prostacyclin analogs for the treatment of PAH and is the only FDA-approved therapy for the treatment of PH-ILD.
Clinical benefits of prostacyclin therapy are well-established and include reduced symptoms of pulmonary hypertension, improved prognostic measures of risk, such as exercise capacity and functional class, and delayed disease progression.4
When inhaled, prostacyclin analogs like treprostinil have the potential to offer substantial benefits over other methods of administration, potentially reducing systemic side effects and providing faster onset than oral formulations.5